Overview 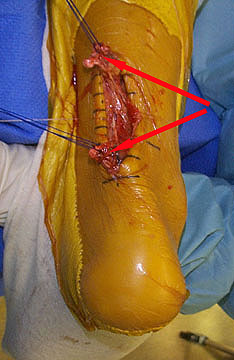 Achilles tendon rupture is when the achilles tendon breaks. The achilles is the most commonly injured tendon. Rupture can occur while performing actions requiring explosive acceleration, such as pushing off or jumping. The male to female ratio for Achilles tendon rupture varies between 7:1 and 4:1 across various studies. Causes Factors that may increase your risk of Achilles tendon rupture include some of the following. Age. The peak age for Achilles tendon rupture is 30 to 40. Sex. Achilles tendon rupture is up to five times more likely to occur in men than in women. Recreational sports. Achilles tendon injuries occur more often during sports that involve running, jumping, and sudden starts and stops, such as soccer, basketball and tennis. Steroid injections. Doctors sometimes inject steroids into an ankle joint to reduce pain and inflammation. However, this medication can weaken nearby tendons and has been associated with Achilles tendon ruptures. Certain antibiotics. Fluoroquinolone antibiotics, such as ciprofloxacin (Cipro) or levofloxacin (Levaquin), increase the risk of Achilles tendon rupture. Symptoms You may notice the symptoms come on suddenly during a sporting activity or injury. You might hear a snap or feel a sudden sharp pain when the tendon is torn. The sharp pain usually settles quickly, although there may be some aching at the back of the lower leg. After the injury, the usual symptoms are as follows. A flat-footed type of walk. You can walk and bear weight, but cannot push off the ground properly on the side where the tendon is ruptured. Inability to stand on tiptoe. If the tendon is completely torn, you may feel a gap just above the back of the heel. However, if there is bruising then the swelling may disguise the gap. If you suspect an Achilles tendon rupture, it is best to see a doctor urgently, because the tendon heals better if treated sooner rather than later. Diagnosis Other less serious causes of pain in the back of the lower leg include Achilles tendonitis or bursitis. To distinguish between these possibilities, your physician will take a thorough history and examine your lower leg to look for signs of a rupture. The presence of a defect in the tendon that can be felt, evidence of weakness with plantarflexion, and a history consistent with Achilles tendon rupture are usually sufficient for diagnosis. Your physician may also perform a ?Thompson test,? which consists of squeezing the calf muscles of the affected leg. With an intact Achilles tendon, the foot will bend downward; however, with a complete rupture of the tendon, the foot will not move. In cases where the diagnosis is equivocal, your physician may order an MRI of the leg to diagnose a rupture of the Achilles tendon. Non Surgical Treatment A medical professional will take MRI scans to confirm the diagnosis and indicate the extent of the injury. Sometimes the leg is put in a cast and allowed to heal without surgery. This is generally not the preferred method, particularly for young active people. Surgery is the most common treatment for an achilles tendon rupture.
Achilles tendon rupture is when the achilles tendon breaks. The achilles is the most commonly injured tendon. Rupture can occur while performing actions requiring explosive acceleration, such as pushing off or jumping. The male to female ratio for Achilles tendon rupture varies between 7:1 and 4:1 across various studies. Causes Factors that may increase your risk of Achilles tendon rupture include some of the following. Age. The peak age for Achilles tendon rupture is 30 to 40. Sex. Achilles tendon rupture is up to five times more likely to occur in men than in women. Recreational sports. Achilles tendon injuries occur more often during sports that involve running, jumping, and sudden starts and stops, such as soccer, basketball and tennis. Steroid injections. Doctors sometimes inject steroids into an ankle joint to reduce pain and inflammation. However, this medication can weaken nearby tendons and has been associated with Achilles tendon ruptures. Certain antibiotics. Fluoroquinolone antibiotics, such as ciprofloxacin (Cipro) or levofloxacin (Levaquin), increase the risk of Achilles tendon rupture. Symptoms You may notice the symptoms come on suddenly during a sporting activity or injury. You might hear a snap or feel a sudden sharp pain when the tendon is torn. The sharp pain usually settles quickly, although there may be some aching at the back of the lower leg. After the injury, the usual symptoms are as follows. A flat-footed type of walk. You can walk and bear weight, but cannot push off the ground properly on the side where the tendon is ruptured. Inability to stand on tiptoe. If the tendon is completely torn, you may feel a gap just above the back of the heel. However, if there is bruising then the swelling may disguise the gap. If you suspect an Achilles tendon rupture, it is best to see a doctor urgently, because the tendon heals better if treated sooner rather than later. Diagnosis Other less serious causes of pain in the back of the lower leg include Achilles tendonitis or bursitis. To distinguish between these possibilities, your physician will take a thorough history and examine your lower leg to look for signs of a rupture. The presence of a defect in the tendon that can be felt, evidence of weakness with plantarflexion, and a history consistent with Achilles tendon rupture are usually sufficient for diagnosis. Your physician may also perform a ?Thompson test,? which consists of squeezing the calf muscles of the affected leg. With an intact Achilles tendon, the foot will bend downward; however, with a complete rupture of the tendon, the foot will not move. In cases where the diagnosis is equivocal, your physician may order an MRI of the leg to diagnose a rupture of the Achilles tendon. Non Surgical Treatment A medical professional will take MRI scans to confirm the diagnosis and indicate the extent of the injury. Sometimes the leg is put in a cast and allowed to heal without surgery. This is generally not the preferred method, particularly for young active people. Surgery is the most common treatment for an achilles tendon rupture.  Surgical Treatment Immediate surgical repair of the tendon is indicated in complete tears. Delaying surgery can lead to shortening of the tendon, formation of scar tissue and decreased blood flow, which can lead to a poor outcome. Following surgery your ankle will be put in an immobilizing device and you will be instructed to use crutches to limit weight bearing and protect the joint. Over the next 2-4 weeks weight bearing will be increased and physical therapy will be initiated. The surgeon will determine the physical therapy timeline and program. Physical Therapy, Treatment will emphasize gradual weaning off the immobilizing device, increased weight bearing, restoration of ankle range of motion and strengthening of the lower leg muscles. It is important that the physician and therapist communicate during the early stages and progress your program based on the principles of healing so as not to compromise the Achilles tendon. Patient will be progressed to more functional activities as normal ankle range of motion and strength is restored.
Surgical Treatment Immediate surgical repair of the tendon is indicated in complete tears. Delaying surgery can lead to shortening of the tendon, formation of scar tissue and decreased blood flow, which can lead to a poor outcome. Following surgery your ankle will be put in an immobilizing device and you will be instructed to use crutches to limit weight bearing and protect the joint. Over the next 2-4 weeks weight bearing will be increased and physical therapy will be initiated. The surgeon will determine the physical therapy timeline and program. Physical Therapy, Treatment will emphasize gradual weaning off the immobilizing device, increased weight bearing, restoration of ankle range of motion and strengthening of the lower leg muscles. It is important that the physician and therapist communicate during the early stages and progress your program based on the principles of healing so as not to compromise the Achilles tendon. Patient will be progressed to more functional activities as normal ankle range of motion and strength is restored.
Achilles tendon rupture is when the achilles tendon breaks. The achilles is the most commonly injured tendon. Rupture can occur while performing actions requiring explosive acceleration, such as pushing off or jumping. The male to female ratio for Achilles tendon rupture varies between 7:1 and 4:1 across various studies. Causes Factors that may increase your risk of Achilles tendon rupture include some of the following. Age. The peak age for Achilles tendon rupture is 30 to 40. Sex. Achilles tendon rupture is up to five times more likely to occur in men than in women. Recreational sports. Achilles tendon injuries occur more often during sports that involve running, jumping, and sudden starts and stops, such as soccer, basketball and tennis. Steroid injections. Doctors sometimes inject steroids into an ankle joint to reduce pain and inflammation. However, this medication can weaken nearby tendons and has been associated with Achilles tendon ruptures. Certain antibiotics. Fluoroquinolone antibiotics, such as ciprofloxacin (Cipro) or levofloxacin (Levaquin), increase the risk of Achilles tendon rupture. Symptoms You may notice the symptoms come on suddenly during a sporting activity or injury. You might hear a snap or feel a sudden sharp pain when the tendon is torn. The sharp pain usually settles quickly, although there may be some aching at the back of the lower leg. After the injury, the usual symptoms are as follows. A flat-footed type of walk. You can walk and bear weight, but cannot push off the ground properly on the side where the tendon is ruptured. Inability to stand on tiptoe. If the tendon is completely torn, you may feel a gap just above the back of the heel. However, if there is bruising then the swelling may disguise the gap. If you suspect an Achilles tendon rupture, it is best to see a doctor urgently, because the tendon heals better if treated sooner rather than later. Diagnosis Other less serious causes of pain in the back of the lower leg include Achilles tendonitis or bursitis. To distinguish between these possibilities, your physician will take a thorough history and examine your lower leg to look for signs of a rupture. The presence of a defect in the tendon that can be felt, evidence of weakness with plantarflexion, and a history consistent with Achilles tendon rupture are usually sufficient for diagnosis. Your physician may also perform a ?Thompson test,? which consists of squeezing the calf muscles of the affected leg. With an intact Achilles tendon, the foot will bend downward; however, with a complete rupture of the tendon, the foot will not move. In cases where the diagnosis is equivocal, your physician may order an MRI of the leg to diagnose a rupture of the Achilles tendon. Non Surgical Treatment A medical professional will take MRI scans to confirm the diagnosis and indicate the extent of the injury. Sometimes the leg is put in a cast and allowed to heal without surgery. This is generally not the preferred method, particularly for young active people. Surgery is the most common treatment for an achilles tendon rupture. Surgical Treatment Immediate surgical repair of the tendon is indicated in complete tears. Delaying surgery can lead to shortening of the tendon, formation of scar tissue and decreased blood flow, which can lead to a poor outcome. Following surgery your ankle will be put in an immobilizing device and you will be instructed to use crutches to limit weight bearing and protect the joint. Over the next 2-4 weeks weight bearing will be increased and physical therapy will be initiated. The surgeon will determine the physical therapy timeline and program. Physical Therapy, Treatment will emphasize gradual weaning off the immobilizing device, increased weight bearing, restoration of ankle range of motion and strengthening of the lower leg muscles. It is important that the physician and therapist communicate during the early stages and progress your program based on the principles of healing so as not to compromise the Achilles tendon. Patient will be progressed to more functional activities as normal ankle range of motion and strength is restored.
